Aortic
Aneurysm Surgery (open/endovascular stenting)
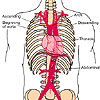
An aneurysm is an abnormal dilation of the vessel
wall. The abnormal swelling can cause symptoms when
it grows, leaks or embolises (showering off debris
from within the vessel). Whilst any vessel can dilate,
most commonly aneurysms form in the abdominal aorta,
the iliac, femoral and popliteal arteries. Occasionally
aneurysms form in the thoracic aorta and carotid
arteries.
Diagnosis
The diagnosis is usually made either by clinical
examination or by ultra sound examination. CT or
MR scanning will give more details about the anatomy
of the AAA (Abdominal Aortic Aneurysm).
Click
on image to enlarge
Indication
for Surgery
The risk of the aneurysm leaking/rupturing has to
be weighed up against the risk of surgery itself.
In small aneurysms (less than about 55mm) the risk
of surgery is usually greater than the risk of observation
alone. Repeat ultrasound examinations at 6 monthly
or yearly intervals allow the rate of growth to
be determined. Over 55mm the risk of rupture is
probably greater than the risk of surgery so surgery
is usually advocated.
Elective vs Emergency Surgery
The risk an elective surgical repair varies from
individual to individual but is usually between
3-7% of a major complication or death. Emergency
repair carries a 50% mortality.
Screening for abdominal aortic aneurysms
There is growing evidence that the introduction
of a population screening programme (in particular
for men) will save lives. Hopefully this will be
introduced into the UK shortly.
Click
on image to enlarge
Open vs Endovascular
Repair
Conventional open surgery on the abdominal aorta
was first undertaken in the 1950s. The operation
is a well tried and tested procedure with good long
term results. Endovascular repair of AAA was first
undertaken in the early 1990s. Its attraction is
the small scars and rapid recovery from surgery.
Unfortunately not all aneuryms are suitable for
an endovascular repair and the long term results
are less well understood. At C&W CVU we work
in close collaboration with our interventional radiologists
and aim to offer the most appropriate approach to
each individual.
Factors Predisposing to Leak or Rupture of Aneurysm
Diameter of aneurysm
Smoking
Diastolic blood pressure
Expansion rate
Family history
Chronic lung disease
Open
Surgery
Click
on image to enlarge
Dacron graft
Top end sewn
into position
Lower anastomosis
complete
Thoracic Aneurysms
Thoracic aneurysms are relative rare. Treatment
options are conservative (leave alone), open surgery
or endovascular surgery. We work closely with our
cardiothoracic colleagues to try to determine the
safest approach.
Click
on image to enlarge
8.5
cms thoracic aneurysm with stent in place
Popliteal Aneurysms
Aneurysmal dilatation can occur in any vessel, but more commonly occurs in the femoral (groin) or popliteal (behind the knee) arteries. Repair is advised before it either leaks or embolizies (showers debris).
Click
on image to enlarge
5cm
popliteal aneurysm with reverse vein graft
Complex visceral
artery reconstructions
Occasionally the renal (kidney) or mesenteric (gut)
arteries narrow or block. Often the best approach
is an endoluminal approach. There are situations
when the endoluminal approach is not possible or
an open approach is more appropriate. The long saphenous
vein (upper thigh) is harvested, reversed and then
used as the conduit.
Click
on image to enlarge
Right
Renal Artery Bypass
Right
renal artery bypass (2)
Aorto-bifem
with left renal artery bypass
Bifurcating
jump vein graft from supra coeliac to common
hepatic and superior mesenteric artery for
mesenteric angina