Carotid
Artery Disease
Background

The blood is supplied to
the brain is via the carotid and vertebral arteries.
There are 130,000 strokes per year in England and
Wales. Between 15-25% of strokes are caused by an
abnormally narrow carotid artery. Platelet debris
can build within an ulcerated plaque. This debris
can be carried by the fast flowing blood in the
artery to the brain causing a transient ischaemic
attack (TIA), mini stroke or stroke.
A TIA (transient ischaemic attack) is a temporary
event in which there is a loss of power or sensation,
loss of speech or loss of vision that lasts less
than 24 hours. A TIA or stroke, caused by a carotid
stenosis, causes a loss of power or sensation that
affects the opposite side of the body to the carotid
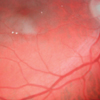
narrowing. However, if the vision is affected by a TIA this occurs on the same side as the stenosis. True visual disturbances caused by TIAs are called Amaurosis Fugax.
| |
|
|
Click
on image to enlarge |
| |
|
|
|
Cholesterol retinal emboli |
| |
|
|
Click
on image to enlarge |
 |
|
|
Carotid angiogram
with stenosis |
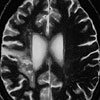
Brain scan
of
patient with stroke |
| |
|
|
|
 |
|
|
Narrowed internal
carotid artery |
Platelet emboli |
Medical treatment
Maximal medical therapy (lowering lipids, controlling
blood pressure, controlling diabetes, and an anti-platelet
drug) is vital and should be started as soon as
possible. It is also crucial to stop smoking. Surgery with maximal medical therapy has been shown to be safer than medical therapy alone in a number of prospective randomised trials.
Investigations
Patients who have had a
TIA or minor stroke should be seen by a specialist
with an interest in TIAs and strokes quickly.
The Royal College of Physicians 2004 Stroke Guidelines
recommends that the patient is seen within 7 days.
Following the index (or first) neurological event,
the risk of a further event is highest in the
first 72 hours.
History, examination and special investigations
should be undertaken. The latter include checking
the blood fat or cholesterol levels and checking
for diabetes. A jelly scan (Duplex) of the neck
vessels should also be performed.
http://www.healthimaging.com/index.php?option=com_articles&view=article&id=5452&division=hiit
The role of surgery
In the 1950s Felix Eastcott reported a case of
a patient with 'recurrent attacks of hemiplegia'
or TIAs who was successfully treated with surgery.
| |
|
|
Click
on image to enlarge |
| |
|
|
|
Eastcott's Lancet Paper |
A number of studies have clearly shown that in
patients with neurological symptoms and a ‘critical
stenosis’ ( >70%) that surgery (carotid
endarterectomy) with drugs is better than drugs
alone at preventing a stroke. This presumes that
the surgical team undertaking the operation is
competent and has a low complication rate.
Recently it has been shown that patients without
symptoms and a critical stenosis may also benefit
from surgery.
The Team
Successful complex surgery involves a large team
of people from a number of disciplines. This starts
with an astute referral from a general practitioner,
an eye specialist or another colleague. Ward nurses,
theatre nurses, high dependency nurses, vascular
technicians, operating department assistants,
anaesthetists, surgeons and not least the patient
each play a vital role in the overall success
rate.
The Operation
In some patients, surgery may be appropriate to
remove the narrowed segment of artery. The aim
of the operation is to restore the narrow artery
to normal, by clearing out the atheroma (narrowing).
If the artery is particularly narrow the vessel
can be widened with a patch made from the patients’s
vein or dacron. The operation can be done under
local or general anaesthesia. The Operation is
usually performed using magnification equipment.
| |
|
|
Click
on image to enlarge |
 |
|
|
| Dacron carotid
patch |
Carotid patch
in situ |
| |
|
|
|
Operating caries a slight risk of a stroke or
heart attack. In most people the risk of having
a stroke is considerably greater if surgery is
not performed. The risks associated with surgery
vary from individual to individual.
In order to operate on the carotid artery it is
necessary to temporarily clamp the artery. In
some patients there is an inadequate collateral
blood supply to the brain and a temporary shunt
(by-pass) needs to be inserted to restore the
blood supply.
| |
|
|
Click
on image to enlarge |
 |
|
|
| Ulcerated plaque |
Shunt in place |
| |
|
|
|
 |
|
|
| Stenotic plaque |
Shunt |
Back
to top
Equipment
Over the years I have found that the standard
carotid clamps do not always allow the best possible
access for surgery. In order to improve access
in such situations, I have designed my own internal
carotid artery clamp that allows access to particularly
high lesions.
| |
|
|
Click
on image to enlarge |
| |
|
|
|
Carotid Clamp |
Crescendo or Recurrent
TIAs and High Risk Carotid Surgery
At the C&W CVU we have pioneered a treatment
for unstable or recurrent TIAs. Following the
first or index event these patients continue to
have further symptoms. This particular group is
at high risk of a further TIA or stroke. In a
proportion of these patients it is possible to
detect clumps of platelets (HITS or high intensity
signals ) in the blood flowing in the brain using
a Trans-Cranial Doppler. Those patients with many
HITS (or a high embolic load) appear to be at
greater risk of having further problems.
It is possible to give drugs to thin the blood
(anti-platelet agents), and it possible to vary
the dose of drug given depending upon the effect
the drugs are having. The treatment involves adjusting
the amount of anti-platelet drugs according to
the number of micro-emboli or HITS detected by
the Trans Cranial Doppler (This is known technically
as TCD-directed anti-platelet therapy). Carotid
surgery can then be safely performed on the next
elective (planned) list.
Control of emboli in patients with recurrent or
crescendo transient ischaemic attacks using preoperative
transcranial Doppler-directed Dextran therapy.
Lennard NS, Vijayasekar C, Tiivas, Chan CWM, Higman
DJ, Imray CHE. British Journal Surgery 2003; 90(2):166-70
Timing of surgery in symptomatic carotid disease.
Imray CHE, Higman DJH, Tiivas C. Lancet 2004;
363(9420):1553-4.
CHE Imray, C Tiivas Are some strokes preventable? A potential role for transcranial Doppler in TIAs of carotid origin. Lancet Neurology 2005; 4(9): 580-6
| |
|
|
Click
on image to enlarge |
 |
|
|
| Platelet aggregates |
Transcranial
Doppler |
| |
|
|
|
| |
|
|
| |
|
Brain scan
of Circle of Willis |
Back to top
Transcranial doppler at high altitude
In an attempt to understand oxygen delivery to the
brain I have combined my carotid interests with my
high altitude interests. The 2007 Caudwell Xtreme
Everest Expedition performed the most extensive
range of physiological tests ever undertaken at high
altitude. We assessed 200 subjects at sea level
(London) and at increasing altitudes to 5,300m
(Everest Base Camp). Climbers underwent testing as
high as the 8,000m (South Col on Everest) in attempt
to investigate how the body responds to exercise in
extreme hypoxia (lack of oxygen).Trans cranial
Doppler and cerebral NIRS (near infrared cerebral
spectroscopy) was performed on five subjects in the
‘death zone’.
http://www.bbc.co.uk/sn/tvradio/programmes/horizon/broadband/tx/everest/
journey/journey_stages/south_col/index.shtml
| |
|
|
Click
on image to enlarge |
 |
|
|
| South Col of
Everest |
Transcranial
Doppler on Everest |
BUPA Stroke Information Sheet
http://hcd2.bupa.co.uk/fact_sheets/html/stroke.html
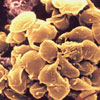
Carotid body tumoursThere is a carotid body on each side of the neck,
and they lie between the internal and external
carotid arteries. CBT are normally small structures
who’s function is to continually measure the oxygen,
carbon dioxide and pH of arterial blood, as a
conseque they have a very rich blood supply.
Tumours can develop in these structures. They tend
to be slow growing and are usually benign, however
if left alone will continue to grow until they cause
local pressure symptoms. CBTs account for
approximately 20% of parapharyngeal tumours in the
west but to up to 80% of this type of tumour at
altitude. CBTs are more common in women than men and
tend to present between 35-50 years of age. Usually
the only symptom is of a swelling in the neck below
the angle of the jaw. A small proportion of the CBTs
secrete catecholamines and will present with raised
blood pressure, racing of the heart, facial flushing
or sweating.
Duplex (ultrasound) scanning, CT and MRI scanning
and occasionally angiography can all assist in
making the diagnosis. CBT will tend to continue to
grow inexorably and are usually best removed
surgically. Sometimes pre-operative embolisation is
advisable to reduce the risk of intra-operative
blood loss. Because of the rich blood supply and
proximity to the major neck arteries and nerves the
procedure should only be undertaken by experienced
carotid surgeons. We routinely use intra-operative
trans cranial Doppler monitoring.
| |
|
|
Click
on image to enlarge |
 |
|
|
| Carotid body
tumour 1 |
Carotid body
tumour 2 |
| |
|
|
|
| |
|
|
| |
|
MRI of
Carotid body tumour |
Combined Coronary Artery and Carotid Artery Disease
Patients undergoing coronary artery surgery have
a small but definite risk of a TIA or stroke. This
risk increases when one or both of the carotid arteries
are narrow or blocked. Working very closely with
cardiology and cardiothoracic colleagues it has
been possible to develop an approach to these high-risk
patients. The carotid surgery is performed under
local anaesthesia prior to the coronary surgery.
We are currently writing up our experience of over
100 combined cases, we believe this is the largest
series to date in the UK.
Ulcerated Plaque
The presence of an ulcerated plaque within the carotid artery appears to increase the risk of further symptoms / TIAs. This needs to be borne in mind when deciding how quickly to operate as this group of patients are at greater risk of a stroke than those in whom no ulcerated plaque is identified.
Trickleflow
Just before a carotid artery blocks, speed of the
blood flowing through the artery may slow to ‘trickle
flow’. At UHCW all patients undergo a repeat
Duplex and TCD immediately prior to surgery. This
is to confirm which side of the neck requires an
operation, the patency of the carotid artery and
to identify the position of the temporal bone window
(natural ‘window’ in the skull through
which the TCD machine can monitor the blood flow
in the middle cerebral artery).
Occlusion
A carotid artery may occasionally block without
symptoms. The risk of further platelet debris passing
up to the brain is virtually nil once this has occurred.
Patients are best treated WITHOUT an operation in
this situation.
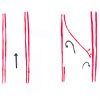
Subintimal Carotid Artery Disection
This is a rare condition that can occur after blunt
trauma to the neck or occasionally it occurs spontaneously
without an apparent cause. The artery splits internally
causing blood to track between the layers of the
blood vessel (see diagram).
This can reduce the blood supply to the brain or
cause platelet debris to shower to brain, both of
which can cause a TIA or stroke.
| |
|
|
Click
on image to enlarge |
 |
|
|
| Subintimal
dissection |
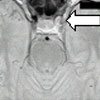
MRA scan showing
reduced diameter of vessel (a) |
| |
|
|
|
| |
|
|
| |
|
MRA scan showing
reduced diameter of vessel (b) |
Back to top
Carotid Stenting
This relatively new technique allows a metal stent
or mesh into the narrowed artery. Theoretical concerns
about the procedure itself causing further debris
or emboli to go to the brain has been partly countered
by the introduction of ‘cerebral protection
devices’. As techniques develop this approach
is likely to be particularly useful in the patient
who is at high risk of open surgery.
| |
|
|
Click
on image to enlarge |
| |
|
|
| |
|
|
|
| |
|
|
|
Hybrid Procedures (subclavian, inominate arteries)
Occasionally there are a
number of narrow arteries that are best dealt with
by a combination of open surgery and endovascular
stenting. A close collaboaration between the surgeon
and interventional radiologist is vital.
| |
|
|
Click
on image to enlarge |
| |
|
|
| |
|
|
|
| |
|
|
|
Subclavian Steal Syndrome
In this relatively rare condition
there is blockage in the artery that supplies the
arm (subclavian). In order for blood to get to the
affected arm it flows up the vertebral artery on
the opposite side and back down the vertebral artery
on the affected side in order to supply the arm.
Treatment is usually via an endovascular approach,
stenting the narrow or occluded subclavian artery.
If the subclavian artery is occluded it is often
helpful to approach the blockage from the affected
arm in addition to the standard groin approach.
Sometimes surgery is required bypassing from the
common carotid to the subclavian artery.
| |
|
|
Click
on image to enlarge |
 |
|
|
| |
|
|
|
| |
|
|
|
 |
|
|
| |
|
|
|
Vertebral Artery Surgery
The vertebral artery, which
supplies the circulation to the back of the brain
(posterior circulation), occasionally narrows. The
narrowing can cause a stroke and occasionally surgery
can be undertaken to prevent further strokes.
In this patient
there was a very tight stenosis at the origin
of the vertebral artery, and the patient had had
a posterior circulation stroke. The vertebral
artery was transposed onto the common carotid
artery.
| |
|
|
Click
on image to enlarge |
 |
|
|
| |
|
|
|
| |
|
|
|
What’s New?
A couple of important papers
have recently been published showing:
1. Carotid surgery in symptomatic patients should
be performed soon after the initial or index event.
Any significant delay to surgery reduces the benefit
of surgery. Ideally patients should have a carotid Duplex scan within 2-7 days of their TIA.
It is suggested that surgery is most beneficial if
performed within 48 hours of the TIA.
2. There is a moderate benefit to undertaking
carotid surgery in patients under 75 who have
not yet had symptoms from their narrow carotids,
so long as their general health is good, and the
hospital where the surgery was to be performed
had good results.
3. The GALA trial (comparing the outcome of carotid
surgery either under general anaesthesia or local
anaesthesia) suggests there is no major
difference between outcomes in LA or GA patients.
4. Carotid stenting may offer an alternative to
open surgery and trials to evaluate the relative
safety of the two approaches continue, but carotid
surgery appears safer in most situations.
5. A number of new antiplatelet agents (both oral
and intravenous) have been introduced and the
full role in the treatment of carotid disease
is being evaluated. Using a combination of aspirin 75mg and Clopidogrel 75mg reduces the platelet microemboli and appears to reduce the risk of a subsequent TIA or stroke in the period immediately after the index or first TIA.
6. Control of platelet emboli both before and
after surgery appears to reduce the risk of stroke.
Few units in the UK currently use these techniques.
A G2b/3a inhibitor Tirofiban may offer an
alternative to Dextran 40 in emboli control.
7. Clopidogrel 75mg the night
before surgery appears to substantially reduce the
risk of post operative embolisation.
8. The trans-orbital
window may offer an alternative to the
trans-temporal window for emboli detection.
Carotid related papers by Chris Imray
Back to top
|
|